How do SGLT2 inhibitors cause DKA?
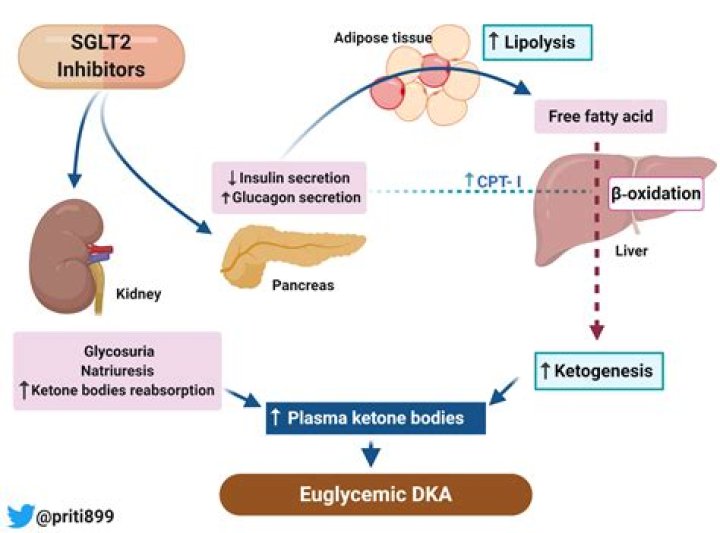
SGLT2 inhibition lowers the renal threshold for glucose excretion, resulting in renal glycosuria, a shift in substrate utilisation from carbohydrate to fat oxidation and hyperglucagonaemia; this poses a theoretical risk for ketoacidosis (including euglycaemic ketoacidosis) in the presence of other precipitating factors …
Why is bicarbonate low in DKA?
Acid–base balance, fluids and electrolytes. Acidosis in DKA is due to the overproduction of β-hydroxybutyric acid and acetoacetic acid. At physiological pH, these 2 ketoacids dissociate completely, and the excess hydrogen ions bind the bicarbonate, resulting in decreased serum bicarbonate levels.
What is the most common cause of diabetic ketoacidosis?
DKA is a state of absolute or relative insulin deficiency aggravated by ensuing hyperglycemia, dehydration, and acidosis-producing derangements in intermediary metabolism. The most common causes are underlying infection, disruption of insulin treatment, and new onset of diabetes.
Why is there hypokalemia in DKA?
DKA is a well-known cause of hypokalemia caused by osmotic diuresis leading to a total body potassium deficiency of 3 to 6 mEq/kg. At presentation, potassium levels are typically “normal” due to the extracellular shift of potassium (K+) from insulin deficiency and acidosis.
Why do SGLT2 inhibitors cause euglycemic DKA?
The pathophysiology of euDKA with SGLT2 inhibitors is thought to involve the lowering of insulin production and increase the glucagon secretion, which promotes a shift of glucose to fat metabolism and stimulates ketogenesis [5,19-20].
What are the first signs that a patient is experiencing diabetic ketoacidosis?
You may notice:
- Excessive thirst.
- Frequent urination.
- Nausea and vomiting.
- Stomach pain.
- Weakness or fatigue.
- Shortness of breath.
- Fruity-scented breath.
- Confusion.
Is diabetic ketoacidosis fatal?
Diabetic ketoacidosis (DKA) is a serious condition that can lead to diabetic coma (passing out for a long time) or even death. When your cells don’t get the glucose they need for energy, your body begins to burn fat for energy, which produces ketones.
What happens to potassium during DKA?
Potassium levels can fluctuate severely during the treatment of DKA, because insulin decreases potassium levels in the blood by redistributing it into cells via increased sodium-potassium pump activity. A large part of the shifted extracellular potassium would have been lost in urine because of osmotic diuresis.
What happens to potassium in metabolic acidosis?
A frequently cited mechanism for these findings is that acidosis causes potassium to move from cells to extracellular fluid (plasma) in exchange for hydrogen ions, and alkalosis causes the reverse movement of potassium and hydrogen ions.
What is diabetic ketoacidosis (DKA)?
Diabetic ketoacidosis (DKA) is a serious complication of diabetes that can be life-threatening. DKA is most common among people with type 1 diabetes. People with type 2 diabetes can also develop DKA. DKA develops when your body doesn’t have enough insulin to allow blood sugar into your cells for use as energy.
Is diabetic ketoacidosis a medical emergency?
Diabetic Ketoacidosis. Elevated ketones are a sign of DKA, which is a medical emergency and needs to be treated right away. Diabetic ketoacidosis (DKA) is a serious complication of diabetes that can be life-threatening. DKA is most common among people with type 1 diabetes.
What is the normal anion gap in diabetic ketoacidosis?
Commonly accepted criteria for diabetic ketoacidosis are blood glucose greater than 250 mg/dl, arterial pH less than 7.3, serum bicarbonate less than 15 mEq/l, and the presence of ketonemia or ketonuria. The normal anion gap is 12 mEq/l. Anion gap greater than 14-15 mEq/l indicates the presence of an increased anion gap metabolic acidosis.
What is the PMCID for adult diabetic ketoacidosis?
PMCID: PMC4085289 PMID: 25061324 Management of adult diabetic ketoacidosis Aidar R Gosmanov,1Elvira O Gosmanova,2and Erika Dillard-Cannon3 Aidar R Gosmanov 1Division of Endocrinology, Diabetes and Metabolism, University of Tennessee Health Science Center, Memphis, TN, USA Find articles by Aidar R Gosmanov Elvira O Gosmanova