What happens to heart rate during orthostatic hypotension?
Both cause dizziness or fainting upon standing. Along with a drop in blood pressure, POTS causes a heart rate increase of 30 to 40 beats per minute within 10 minutes of standing.
Does systolic blood pressure drop standing?
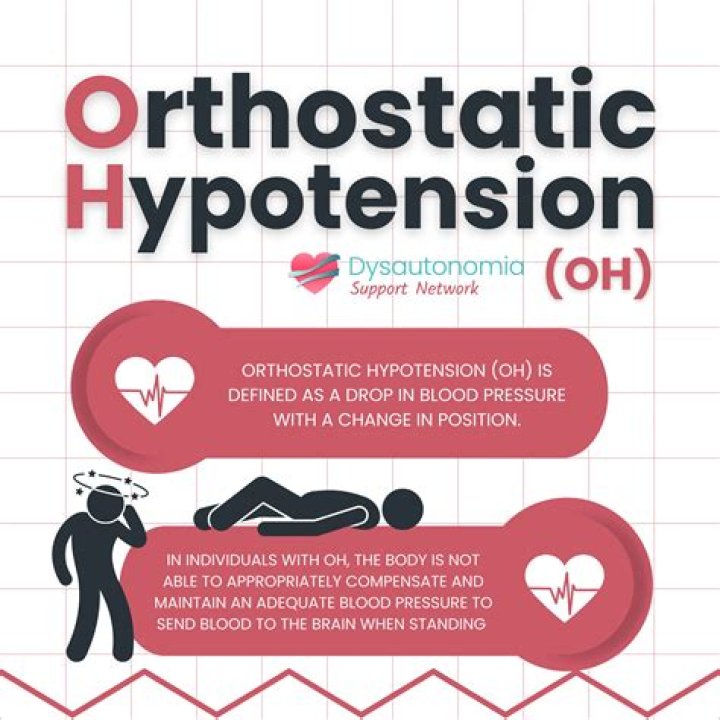
Orthostatic hypotension (OH), defined as a systolic blood pressure (SBP) drop of 20 mm Hg or a diastolic blood pressure (DBP) drop of 10 mm Hg within 3 minutes after standing up, occurs in 5% to 30% of adults above 65 years of age and is associated with impaired physical and cognitive functioning, cardiovascular …
Is orthostatic hypotension life-threatening?
In people with orthostatic hypotension, hypoperfusion to other organs contributes to an increased risk of life-threatening health problems, including heart attack or heart failure, a heart rhythm abnormality called atrial fibrillation , stroke, or chronic kidney failure.
Is orthostatic hypotension life threatening?
Is orthostatic hypertension life-threatening?
Should I be worried about orthostatic hypotension?
Orthostatic hypotension may be mild, and episodes can last for less than a few minutes. However, long-lasting orthostatic hypotension can signal more-serious problems, so it’s important to see a doctor if you frequently feel lightheaded when standing up.
How dangerous is orthostatic hypotension?
Orthostatic hypotension may cause dizziness or a loss of consciousness, causing the person to faint or pass out. It can occur within three minutes of standing up. Orthostatic hypotension can be dangerous, as it can put the person in serious risk of falls and injury.1.
How to assess orthostatic hypotension?
A new study led by Johns Hopkins researchers suggests that testing for the presence of orthostatic hypotension, a form of low blood pressure, be performed within one minute of standing after a person has been lying down. Current guidelines recommend taking the measurement three minutes after a person stands up.
What is the best medication for systolic hypertension?
The data so far available indicate that low‐dose thiazide diuretics and slow/long‐acting calcium antagonists are the drugs of first choice. A slow reduction of systolic pressure in the mostly elderly patients is mandatory. A target level of SBP around 140 mmHg seems desirable.